
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamapediatrics/fullarticle/10.1001/jamapediatrics.2019.3939?guestAccessKey=3cfb13d2-3d7f-4763-90bd-d1aec82bb2ca&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102819
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamasurgery/fullarticle/10.1001/jamasurg.2019.4702?guestAccessKey=6c0b80f5-293b-4f90-ad1f-f50c066f1f5d&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102819
Childhood Cancer Survivors and Later Breast Cancer Risk
JAMA Pediatrics
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 28, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamapediatrics/fullarticle/10.1001/jamapediatrics.2019.3807?guestAccessKey=92330737-9acb-43ca-85ed-c07b1be7dfb5&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102819
What The Study Did: This study examined later breast cancer risk in childhood cancer survivors following radiation and chemotherapy treatment.
Author: Lena H. Veiga, Ph.D., of the National Cancer Institute in Bethesda, Maryland, is the corresponding author.
(doi:10.1001/jamapediatrics.2019.3807)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Did Banning Sugar-Sweetened Drinks at Work Cut Employee Consumption?
JAMA Internal Medicine
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 28, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/10.1001/jamainternmed.2019.4434?guestAccessKey=c104b006-fa16-4100-824e-a4e9af86af07&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102819
What The Study Did: This study examined the effects of a workplace ban on sales of sugar-sweetened beverages on employee consumption and health.
Authors: Elissa S. Epel. Ph.D., of the University of California, San Francisco, is the corresponding author.
(doi:10.1001/jamainternmed.2019.4434)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
What Are Encounters With Biased Patients Like for Physicians?
JAMA Internal Medicine
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 28, 2019
Media advisory: The full study, commentary and podcast are linked to this news release.
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/10.1001/jamainternmed.2019.4122?guestAccessKey=547e97c5-3be3-462f-a79e-48d53f162de3&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102819
What The Study Did: A group of 50 nonwhite hospitalist attending physicians, internal medicine residents and medical students described their encounters with biased patients (ranging from patients refusing care to explicit racist, sexist or homophobic comments and belittling jokes) in this qualitative study to understand physicians’ perspectives on these encounters, which could help in the development of best practices and training programs at institutions as the clinical workforce becomes more diverse.
Authors: Alicia Fernandez, M.D., of the University of California, San Francisco, is the corresponding author.
(doi:10.1001/jamainternmed.2019.4122)
Editor’s Note: The article contains funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamaoncology/fullarticle/10.1001/jamaoncol.2019.4107?guestAccessKey=31572357-2b2d-4b00-ba8e-ff65e337922e&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102419
Detection of Oral HPV DNA in Teen, Young Adult Females
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), FRIDAY, OCTOBER 25, 2019
Media advisory: To contact corresponding author Nicolas F. Schlecht, Ph.D., email Annie Deck-Miller at annie.deck-miller@roswellpark.org. The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.14031?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=102519
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
Bottom Line: Researchers tested for HPV DNA in oral rinse samples collected over 10 years from a group of sexually active females (ages 13 to 21) who were planning to or had received the vaccine that targets four types of HPV. HPV was detected in 6.2% of 1,259 participants at baseline but oral HPV detection became less likely with time since becoming sexually active. And, researchers report detection of the HPV types targeted by the vaccine was even less likely among those who received at least one dose of the vaccine compared with those who were fully unvaccinated. Study cohort characteristics include a population that had more sexual partners and an earlier initiation of sexual activity than other groups that have been studied. HPV is a common sexually transmitted infection that is associated with increased risk of some cancers, including in the oral cavity.
Authors: Nicolas F. Schlecht, Ph.D., of the Roswell Park Comprehensive Cancer Center, Buffalo, New York, and coauthors
(doi:10.1001/jamanetworkopen.2019.14031)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Length of Time in US Associated With Immigrants’ Opioid Use
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), FRIDAY, OCTOBER 25, 2019
Media advisory: To contact corresponding author Brian D. Sites, M.D., M.S., email Audra Burns at Audra.Burns@hitchcock.org. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.13979?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=102519
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
Bottom Line: The more time first-generation immigrants spend in the United States the more likely it appears they will use prescription opioids. This analysis used nationally representative survey data on health services that include prescription medications and self-reported length of time spent in the country. Among an estimated 41.5 million adult immigrants living in the United States, 3.2 million (7.8%) use prescription opioids. Study authors report the rate of opioid use increased from 4.7% among new immigrants (less than five years in the U.S.) to 14.8% among long-standing immigrants (in the U.S. 15 years or more). Nonimmigrants were more likely to use prescription opioids compared with all first-generation immigrants (16.1% vs. 7.8%). The findings suggest uniquely American cultural factors may promote opioid use.
Authors: Brian D. Sites, M.D., M.S., Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire, and coauthors
(doi:10.1001/jamanetworkopen.2019.13979)
Editor’s Note: The article includes conflict of interest disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
How is Physical Activity Associated With Fracture Risk in Older Women?
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), FRIDAY, OCTOBER 25, 2019
Media advisory: The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.14084?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=102519
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
What The Study Did: In this observational study of 77,206 postmenopausal women, researchers looked at how physical activity and sedentary behavior were associated with risk of fracture.
Authors: Jean Wactawski-Wende, Ph.D., of the University at Buffalo in New York, is the corresponding author.
(doi:10.1001/jamanetworkopen.2019.14084)
Editor’s Note: The article contains funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
How Did Weight-Loss Surgery Affect Long-Term Health Care Expenses?
JAMA Surgery
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 30, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamasurgery/fullarticle/10.1001/jamasurg.2019.3732?guestAccessKey=7aa8ca1a-316f-44b0-9239-5a3ae22cbfe6&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=103019
What The Study Did: This observational study of nearly 10,000 veterans with severe obesity compared health care expenditures for veterans who had weight-loss surgery with those who didn’t during up to 10 years of follow-up.
Authors: Matthew L. Maciejewski, Ph.D., of the Durham VA Medical Center in Durham, North Carolina, is the corresponding author.
(doi:10.1001/jamasurg.2019.3732)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Study Examines Fetal Exposure to Acetaminophen, Risk of Childhood ADHD, ASD
JAMA Psychiatry
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 30, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamapsychiatry/fullarticle/10.1001/jamapsychiatry.2019.3259?guestAccessKey=83e36a6e-f239-43f0-9c6e-9983db4436d0&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=103019
What The Study Did: Umbilical cord blood samples were used to examine an association between fetal exposure to acetaminophen and risk of childhood attention-deficit/hyperactivity disorder, autism spectrum disorder and other developmental disabilities in a group of nearly 1,000 mother-child pairs.
Authors: Xiaobin Wang, M.D., M.P.H., Sc.D., of the Johns Hopkins University Bloomberg School of Public Health in Baltimore, is the corresponding author.
(doi:10.1001/jamapsychiatry.2019.3259)
Editor’s Note: The article contains funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Is Weight Loss Surgery Associated With a Reduced Risk of Skin Cancer?
JAMA Dermatology
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 30, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamadermatology/fullarticle/10.1001/jamadermatol.2019.3240?guestAccessKey=8d3a865d-9619-4640-a9ee-a47149039d91&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=103019
What The Study Did: Researchers investigated the association between weight loss surgery and a subsequent diagnosis of skin cancer, including melanoma, among 4,000 obese patients in Sweden, who had the surgery or received usual treatment.
Authors: Magdalena Taube, Ph.D., of the University of Gothenburg, in Gothenburg, Sweden, is the corresponding author.
(doi:10.1001/jamadermatol.2019.3240)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
How Common is Pain in Kids, Teens With ASD?
JAMA Pediatrics
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 28, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamapediatrics/fullarticle/10.1001/jamapediatrics.2019.3826?guestAccessKey=fdb5efdd-1bbf-460b-a122-d4e205eddc37&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102819
What The Study Did: Survey responses from parents were used to assess how often children and teens (ages 6 to 17) with autism spectrum disorders (ASD) had repeated or chronic physical pain in the previous 12 months compared to children without ASD.
Authors: Daniel G. Whitney, Ph.D., and Danielle N. Shapiro, Ph.D.,of the University of Michigan in Ann Arbor, are the authors.
(doi:10.1001/jamapediatrics.2019.3826)
Editor’s Note: The article contains conflict of interest disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Dementia, Alzheimer Disease in People With Down Syndrome
JAMA Neurology
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 28, 2019
Media Advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamaneurology/fullarticle/10.1001/jamaneurol.2019.3666?guestAccessKey=32ec26cb-4f2f-4cde-aca9-87927ec2c770&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102819
What The Study Did: Medicaid claims data in Wisconsin were analyzed to examine how common dementia and Alzheimer disease were in people with Down syndrome because clinical studies show them to be at higher risk and to have an earlier onset of dementia.
Authors: Eric Rubenstein, Ph.D., of the University of Wisconsin-Madison, is the corresponding author.
(doi:10.1001/jamaneurol.2019.3666)
Editor’s Note: The article includes funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Study Examines First Use of Flavored Tobacco Products
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 23, 2019
Media advisory: The full study is linked to this news release and a visual abstract is below.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.13804?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=102319
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
What The Study Did: Associations between the first use of flavored tobacco products and subsequent use of those products were examined in this observational study based on nationally representative survey data of more than 38,400 youth and adults in the United States.
Authors: Andrea C. Villanti, Ph.D., M.P.H., of the University of Vermont in Burlington, is the corresponding author.
Visual Abstract:

(doi:10.1001/jamanetworkopen.2019.13804)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Increase in Older Adults in US Associated With Increase in Heart Disease Deaths
JAMA Cardiology
EMBARGOED FOR RELEASE: 1:05 A.M. (ET), WEDNESDAY, OCTOBER 30, 2019
Media advisory: To contact corresponding author Stephen Sidney, M.D., M.P.H., email Janet Byron at Janet.L.Byron@kp.org. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamacardiology/fullarticle/10.1001/jamacardio.2019.4187?guestAccessKey=7c7fe675-8c73-4065-a36e-898696329c13&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=103019
Bottom Line: An increase in the number of U.S. adults 65 and older from 2011 to 2017 was associated with an increase in heart disease deaths in that age group despite a slowly declining heart disease mortality rate in the total population. Data from the U.S. Centers for Disease Control and Prevention and the Census Bureau were used to examine changes in heart disease deaths in combination with demographic changes in the population in this observational study. Authors report the 65-and-older population grew from 41.4 million to 50.9 million from 2011 to 2017, an increase of nearly 23%, while the adult population younger than 65 grew by only 1.7%. The overall mortality rate from all heart disease adjusted to account for differences in age declined 5% while the total number of deaths increased 8.5%, with 80% of the deaths among adults 65 and older. Deaths from all heart disease increased 5.7% from 2011 to 2017 among adults younger than 65 but increased 9.3% among those 65 and older. From 2011 t02017, the overall age-adjusted mortality rate from coronary heart disease decreased 14.9% but increased 20.7% from heart failure as the underlying cause. Limitations of the study include the potential misclassification of death certificate coding of heart failure and limitations of national surveillance data. The authors stress that with the number of adults 65 and older projected to increase another 44% in the U.S. from 2017 to 2030, innovative and effective approaches to prevent and treat heart disease are needed.
Authors: Stephen Sidney, M.D., M.P.H., of Kaiser Permanente Northern California, Oakland, and coauthors.
(doi:10.1001/jamacardio.2019.4187)
Editor’s Note: The article includes conflict of interest disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Increasing Google Searches for Marijuana Chemical Component CBD
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 23, 2019
Media advisory: To contact corresponding author John W. Ayers, Ph.D., M.A., email Louise Canton at louise@elevatedsciencecommunications.com. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.13853?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=102319
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
Bottom Line: Google searches from 2004 through April 2019 were used to measure U.S. public interest in cannabidiol (CBD), a chemical component of marijuana. Searches from the United States that mentioned “CBD” or “cannabidiol” were stable from 2004 through 2014 before substantial increases in search volumes of almost 126% in 2017 compared with 2016 and 160% during 2018 compared with 2017. There were 6.4 million Google searches for CBD during April 2019 and year-over-year forecasted search volumes are expected to increase nearly 118% during 2019 compared with 2018. A limitation of this observational study is that Google searches may reflect interest in CBD rather than interest in its use. Researchers urge that attention to CBD be a public health priority because of the growing interest that surrounds it to understand who uses it and why, and to evaluate its effects and potential drug interactions.
Authors: John W. Ayers, Ph.D., M.A., University of California San Diego, and coauthors
(doi:10.1001/jamanetworkopen.2019.13853)
Editor’s Note: The article includes conflict of interest disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Is Parental Income During Childhood Associated With Kids’ Later Schizophrenia Risk?
JAMA Psychiatry
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 23, 2019
Media advisory: The full study and editorial are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamapsychiatry/fullarticle/10.1001/jamapsychiatry.2019.2299?guestAccessKey=fe6e8805-e2de-4902-9c7b-06159dc53293&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102319
What The Study Did: Researchers analyzed data from everyone born in Denmark from 1980-2000 to look at associations between parental income until children are 15 and the risk of schizophrenia later in life for children.
Authors: Christian Hakulinen, Ph.D., of the University of Helsinki in Finland, is the corresponding author.
(doi:10.1001/jamapsychiatry.2019.2299)
Editor’s Note: The article includes funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
How Much Cardiovascular Disease Among Black Adults is Attributable to Hypertension?
JAMA Cardiology
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 23, 2019
Media advisory: To contact corresponding author Donald Clark III, M.D., M.P.H., email Annie Oeth at aoeth@umc.edu. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamacardiology/fullarticle/10.1001/jamacardio.2019.3773?guestAccessKey=9c5bc61e-ebca-4e25-8d88-ff077a402bdb&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102319
Bottom Line: Estimating the proportion of cardiovascular disease (CVD) cases among black adults associated with hypertension was the focus of this observational study. The analysis included data on nearly 12,500 black adults in the United States, of whom 9,633 had hypertension. Researchers calculated population-attributable risk, which represents the proportion of cases of a disease in a population attributed to a risk factor. The findings suggest nearly one-third (32.5%) of CVD cases were associated with hypertension. Interventions to maintain normal blood pressure throughout life may help reduce CVD among black adults. A limitation of the study is that a common risk factor, such as hypertension, can make estimates of population-attributable risk less precise.
Authors: Donald Clark III, M.D., M.P.H., of the University of Mississippi Medical Center, Jackson, and coauthors.
(doi:10.1001/jamacardio.2019.3773)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
English Proficiency Associated With Hospital Revisits, Readmissions
JAMA
EMBARGOED FOR RELEASE: 11 A.M. (ET), TUESDAY, OCTOBER 22, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.13066?guestAccessKey=776f620c-15cf-4df6-b98a-cb57bdc28a20&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102219
What The Study Did: Patients with limited English proficiency face barriers in health care settings. This observational study examined whether return emergency department visits or hospital readmissions differed between English-proficient patients and those with limited proficiency who were discharged with acute (pneumonia and hip fracture) and chronic (chronic obstructive pulmonary disease and heart failure) conditions from two Toronto hospitals.
Authors: Shail Rawal, M.D., M.P.H., of the University of Toronto, is the corresponding author.
(doi:10.1001/jama.2019.13066)
Editor’s Note: The article includes funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamapediatrics/fullarticle/10.1001/jamapediatrics.2019.3804?guestAccessKey=28c20609-a669-4a04-9ee3-2af51c7a2551&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102119
Trial Compares SSRI vs. Placebo for Obsessive-Compulsive Behaviors in Kids, Teens With ASD
JAMA
EMBARGOED FOR RELEASE: 11 A.M. (ET), TUESDAY, OCTOBER 22, 2019
Media advisory: To contact corresponding author Dinah S. Reddihough, M.D., email dinah.reddihough@rch.org.au. The full study and editorial are linked to this news release. A visual abstract is below.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.14685?guestAccessKey=51958aff-a578-4f40-8196-0293f4d957b7&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102219
Bottom Line: Researchers compared the selective serotonin reuptake inhibitor (SSRI) fluoxetine with placebo for reducing the frequency and severity of obsessive-compulsive behaviors in children and adolescents with autism spectrum disorder (ASD) in this randomized clinical trial in Australia. The trial included 146 participants (ages 7 to 18) with ASDs; 75 received fluoxetine and 71 received placebo for 16 weeks. Of the participants, 109 completed the trial. The authors report that for the primary outcome (total scores on an obsessive-compulsive scale modified for pervasive developmental disorder) treatment with fluoxetine compared with placebo resulted in lower scores for obsessive-compulsive behaviors but the interpretation of that finding is limited by a number of factors. These factors include the study’s high dropout rate and significant differences found between groups in some measures at baseline.
Authors: Dinah S. Reddihough, M.D., of the Royal Children’s Hospital, Melbourne, Australia, and coauthors.
(doi:10.1001/jama.2019.14685)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Clinical Trial in Japan Focuses on Avoiding Cow’s Milk Formula to Supplement Breastfeeding
JAMA Pediatrics
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 21, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamapediatrics/fullarticle/10.1001/jamapediatrics.2019.3544?guestAccessKey=642cb0c8-a18e-4ee1-80bf-56994efc073c&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102119
What The Study Did: A randomized clinical trial in Japan with about 300 newborns looked at whether avoiding cow’s milk formula to supplement breastfeeding would decrease risks of sensitization to cow’s milk protein or food allergy, including cow’s milk allergy.
Author: Mitsuyoshi Urashima, M.D., M.P.H., Ph.D., of the Jikei University School of Medicine in Tokyo, is the corresponding author.
(doi:10.1001/jamapediatrics.2019.3544)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Analysis of US Pharmacy Closures
JAMA Internal Medicine
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 21, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/10.1001/jamainternmed.2019.4588?guestAccessKey=9f0d3d86-193b-40b4-a8de-5d015f8842ab&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102119
What The Study Did: This research letter reports on pharmacy closures in the United States and risk factors associated with closure.
Authors: Dima M. Qato, Pharm.D., M.P.H., Ph.D., of the University of Illinois at Chicago, is the corresponding author.
(doi:10.1001/jamainternmed.2019.4588)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Is Cigarette Type Associated With Lung Cancer Outcomes?
JAMA Internal Medicine
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 21, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/10.1001/jamainternmed.2019.3487?guestAccessKey=40e559a5-e128-4289-b617-a70f476d7dee&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102119
What The Study Did: An association between lung cancer outcomes and the filter status of cigarettes, their tar level and menthol flavor was examined using data from more than 14,000 participants in a lung screening trial who completed detailed questionnaires about smoking.
Authors: Nichole T. Tanner, M.D., M.S.C.R., of the Ralph H. Johnson Veterans Affairs Hospital in Charleston, South Carolina, is the corresponding author.
(doi:10.1001/jamainternmed.2019.3487)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Born Premature, How Common to be Adult With No Major Health Conditions?
JAMA
EMBARGOED FOR RELEASE: 11 A.M. (ET), TUESDAY, OCTOBER 22, 2019
Media advisory: To contact corresponding author Casey Crump, M.D., Ph.D., email Tildy La Farge at Tildy.lafarge@mountsinai.org. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.15040?guestAccessKey=001a2beb-213b-4149-92e0-b4d852bf2b94&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=102219
Bottom Line: This observational study looked at how common it was for people born premature to become adults without any major health conditions such as asthma, hypertension, diabetes and epilepsy, all of which have been associated with preterm birth. This analysis included birth registry data in Sweden for more than 2.5 million people born from 1973 to 1997, of whom 149,065 were born preterm (gestational age less than 37 weeks). Of all those born preterm, 54.6% were alive with no major medical conditions at ages 18 to 43 compared with 63% of people born at full-term. Limitations of the study include that detailed clinical data weren’t available to validate health conditions and longer follow-up is needed to examine outcomes after the age of 43.
Authors: Casey Crump, M.D., Ph.D., Icahn School of Medicine at Mount Sinai, New York, and coauthors.
(doi:10.1001/jama.2019.15040)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
New Video Accompanies Article About Waste in US Health Care System
JAMA
FOR IMMEDIATE RELEASE: Tuesday, October 15, 2019
Media advisory: To contact corresponding author William H. Shrank, M.D., M.S.H.S., email Alex Kepnes at akepnes@humana.com. The full study, editorials, summary video and podcast are linked to this news release. The video can be viewed on this page and embedded on your website by copying and pasting the HTML code below.
Embed this link to provide your readers free access to the full-text article https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.13978?guestAccessKey=bf8f9802-be69-4224-a67f-42bf2c53e027&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100719
Bottom Line: A new study estimates about one-quarter of total health care spending in the United States is waste, with a price tag ranging from $760 billion to $935 billion. The United States spends more on health care than any other country. For this analysis, the authors identified government-based reports, articles and peer-reviewed publications from 2012 to 2019 that focused on estimates of costs or savings related to six areas of waste. There were 71 estimates from 54 publications and those estimates were combined into ranges or totaled. Study authors report total estimated annual cost of waste was $265.6 billion for administrative complexity (billing and coding waste, physician time spent reporting on quality measures); $230.7 billion to $240.5 billion for pricing failure (prices increase far from those expected in a well-functioning market); $102.4 billion to $165.7 billion for failure of care delivery (poor execution or lack of widespread adoption of best care processes); $75.7 billion to $101.2 billion for overtreatment or low-value care; $58.5 billion to $83.9 billion for fraud and abuse; and $27.2 billion to $78.2 billion for failure of care coordination (unnecessary admissions or avoidable complications and readmissions). The authors also searched the published literature to find estimates of the potential to reduce waste in each of the categories listed by scaling proven strategies. Projected potential savings from efforts to reduce waste ranged from $191 billion to $282 billion, a potential 25% reduction in the total cost of waste. The authors highlight the opportunity to reduce waste through insurer-clinician collaboration and data interoperability. This analysis has limitations, including that the studies used may not represent all costs and savings in each area of waste, and that data from some of the studies may not be generalizable to the U.S. population. Implementing effective measures to decrease waste is a chance to reduce continued increases in U.S. health care costs.
Authors: William H. Shrank, M.D., M.S.H.S., Humana Inc., Louisville, Kentucky, and coauthors
Video embed code:
(doi:10.1001/jama.2019.13978)
Editor’s Note: The article includes conflict of interest disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Aspirin Use After Biliary Tract Cancer Diagnosis
JAMA Oncology
EMBARGOED FOR RELEASE: 11 A.M. (ET), THURSDAY, OCTOBER 17, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamaoncology/fullarticle/10.1001/jamaoncol.2019.4328?guestAccessKey=4b431465-c9dc-4248-b994-80f4c972fac7&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101719
What The Study Did: Researchers in this observational study examined if aspirin use after a diagnosis of a biliary tract cancer, which includes gallbladder cancer, was associated with reduced risk of death among nearly 3,000 patients.
Authors: Sarah S. Jackson, Ph.D., of the National Cancer Institute in Rockville, Maryland, is the corresponding author.
(doi:10.1001/jamaoncol.2019.4328)
Editor’s Note: The article includes funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Examining Depression, Postoperative Regret After Major Head/Neck Surgery
JAMA Otolaryngology-Head & Neck Surgery
EMBARGOED FOR RELEASE: 11 A.M. (ET), THURSDAY, OCTOBER 17, 2019
Media advisory: The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamaotolaryngology/fullarticle/10.1001/jamaoto.2019.3020?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101719
What The Study Did: Researchers investigated whether frail or elderly patients with head and neck cancer have worse depression or higher rates of regret after surgery.
Authors: David P. Goldstein, M.D., M.Sc., of the University of Toronto, is the corresponding author.
(doi:10.1001/jamaoto.2019.3020)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Is Exposure to Disinfectants, Cleaning Products at Work Associated With COPD Among Female Nurses?
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), FRIDAY, OCTOBER 18, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.13563?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=101819
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
What The Study Did: This observational study investigated an association between exposure to disinfectants and cleaning products at work and risk of new cases of chronic obstructive pulmonary disease (COPD) among a large group of female nurses.
Authors: Orianne Dumas, Ph.D., of INSERM U1168, VIMA: Aging and Chronic Diseases, Epidemiological and Public Health Approaches in Villejuif, France, is the corresponding author.
(doi:10.1001/jamanetworkopen.2019.13563)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Exposure to Secondhand Smoke Associated With Eye Differences Among Children
JAMA Ophthalmology
EMBARGOED FOR RELEASE: 11 A.M. (ET), THURSDAY, OCTOBER 17, 2019
Media advisory: The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamaophthalmology/fullarticle/10.1001/jamaophthalmol.2019.4178?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101719
What The Study Did: About 1,400 young children in Hong Kong had eye exams to see if those exposed to secondhand smoke at home had differences in choroidal thickness, a layer of the eye that contains blood vessels and connective tissue, compared to children not exposed to smoke.
Authors: Jason C. Yam, F.R.C.S.Ed., of the Chinese University of Hong Kong, is the corresponding author.
(doi:10.1001/jamaophthalmol.2019.4178)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Changes in Cardiovascular Risk Factors Among College Football Players
JAMA Cardiology
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 16, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamacardiology/fullarticle/10.1001/jamacardio.2019.3909?guestAccessKey=a6e0736c-a9a1-408f-b0e9-c519343b71ba&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101619
What The Study Did: Researchers recruited 126 college football players from two programs in Georgia and South Carolina to examine over three years how cardiovascular risk factors emerged and changed, including weight, blood pressure and heart structure and function.
Authors: Jonathan H. Kim, M.D., M.Sc., of the Emory Clinical Cardiovascular Research Institute in Atlanta, is the corresponding author.
(doi:10.1001/jamacardio.2019.3909)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Do Surgeons Get Lower Patient Satisfaction Ratings When They Prescribe Fewer Opioids?
JAMA Surgery
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 16, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamasurgery/fullarticle/10.1001/jamasurg.2019.2875?guestAccessKey=aab5adb4-52a6-4470-bcec-426257e6a9d2&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101619
What The Study Did: A survey study of nearly 1,000 patients who underwent common outpatient surgical procedures reports no significant change in ratings for how satisfied patients were with surgeons when surgeons prescribed fewer opioids.
Authors: Richard J. Barth Jr., M.D., of the Dartmouth-Hitchcock Medical Center in Lebanon, New Hampshire, is the corresponding author.
(doi:10.1001/jamasurg.2019.2875)
Editor’s Note: Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Sociodemographic Factors Associated With Passing Surgery Board Exams
JAMA Surgery
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 16, 2019
Media advisory: The full study, commentary and podcast are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamasurgery/fullarticle/10.1001/jamasurg.2019.4081?guestAccessKey=00a8ee32-a0f4-4591-a43f-3db5ffb18b9a&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101619
What The Study Did: Survey responses from general surgery trainees were used to examine the association between sociodemographic factors such as race/ethnicity, gender and family status with the likelihood of passing the American Board of Surgery board examinations.
Authors: Heather L. Yeo, M.D., M.H.S., M.B.A., M.S., of NewYork-Presbyterian/Weill Cornell Medicine in New York City, is the corresponding author.
(doi:10.1001/jamasurg.2019.4081)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Examining Risk of Suicide and Use of ACE Inhibitors, ARBs
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 16, 2019
Media advisory: The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.13304?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=101619
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
What The Study Did: Associations between risk of suicide and medications widely used in the management of high blood pressure, chronic kidney disease, heart failure and diabetes (angiotensin-converting enzyme inhibitors and angiotensin receptor blockers) were examined in this observational study.
Authors: Tony Antoniou, Pharm.D., Ph.D., of St. Michael’s Hospital in Toronto, is the corresponding author.
(doi:10.1001/jamanetworkopen.2019.13304)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Here’s a link to provide your readers free access to the full-text article
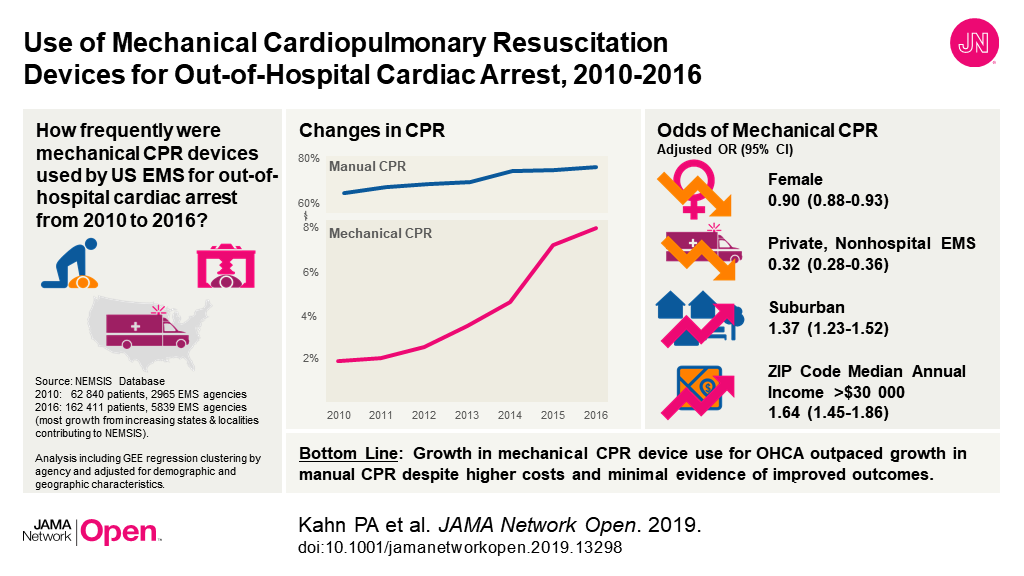
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.13298?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=101619
Visual Abstract
Study Examines Breastfeeding and Risk of Maternal Diabetes, Hypertension
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 16, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.13401?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=101619
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
What The Study Did: To examine if breastfeeding is associated with a lower risk of maternal diabetes or hypertension, six studies with more than 200,000 participants were combined in this systematic review and meta-analysis.
Authors: Haitham M. Ahmed, M.D., M.P.H., of AdvantageCare Physicians in New York, is the corresponding author.
(doi:10.1001/jamanetworkopen.2019.13401)
Editor’s Note: Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Psoriasis Appears Associated With Increased Risk of Developing, Dying of Cancer
JAMA Dermatology
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 16, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamadermatology/fullarticle/10.1001/jamadermatol.2019.3056?guestAccessKey=c91d53c0-6564-4c0f-9465-d941756c3bb3&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101619
What The Study Did: The risk of developing and dying of cancer among people with psoriasis was examined in this study (called a systematic review and meta-analysis) that combined the results of 58 observational studies.
Authors: Alex M. Trafford, M.Sc., of the University of Manchester in the United Kingdom, is the corresponding author.
(doi:10.1001/jamadermatol.2019.3056)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Are High School Personality Traits Associated With Later Dementia Diagnoses?
JAMA Psychiatry
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 16, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamapsychiatry/fullarticle/10.1001/jamapsychiatry.2019.2914?guestAccessKey=0c3f389d-11cb-4b6a-9a2f-802e5672524e&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101619
What The Study Did: A national sample of high school students in the United States in 1960 was used in this observational study to assess whether personality traits measured in high school were associated with dementia diagnoses more than 50 years later using Medicare records.
Authors: Benjamin P. Chapman, Ph.D., M.P.H., M.S., of the University of Rochester Medical Center in Rochester, New York, is the corresponding author.
(doi:10.1001/jamapsychiatry.2019.2914)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Bulimia Nervosa and Long-Term Risk of Cardiovascular Disease, Death Among Women
JAMA Psychiatry
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 16, 2019
Media advisory: The full study and editorial are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamapsychiatry/fullarticle/10.1001/jamapsychiatry.2019.2914?guestAccessKey=1e6086ce-a6d1-4632-95ca-39b649d31075&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101619
What The Study Did: Bulimia nervosa (binge eating followed by purging) is a common psychiatric disease in women. This observational study examined the association between bulimia nervosa and the risk of long-term cardiovascular disease and death during 12 years of follow-up using hospitalization data for a large group of women in Canada.
Authors: Nathalie Auger, M.D., M.Sc., F.R.C.P.C., of the Institut National de Santé Publique du Québec in Canada, is the corresponding author.
(doi:10.1001/jamapsychiatry.2019.2914)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.14630?guestAccessKey=28863035-c5ce-4c2d-8ec7-3a2e7121774c&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101519
Is Bipolar Disorder Associated With Increased Risk of Parkinson Disease?
JAMA Neurology
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 14, 2019
Media Advisory: To contact corresponding author Joaquim J. Ferreira, M.D., Ph.D., email joaquimjferreira@gmail.com. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamaneurology/fullarticle/10.1001/jamaneurol.2019.3446?guestAccessKey=2cb24d8a-f8cf-4e48-b523-7ac94ff8a6b9&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101419
Bottom Line: This study, called a systematic review and meta-analysis, combined the results of seven studies with 4.3 million participants to examine a potential association between bipolar disorder with a later diagnosis of Parkinson disease of unknown cause. The findings suggest that a previous diagnosis of bipolar disorder was associated with increased likelihood of a subsequent Parkinson disease diagnosis but subgroup analyses suggest the possibility of an overestimation of the magnitude of the associations. The main limitation of the study is analysis that suggests a greater likelihood of a Parkinson disease diagnosis in shorter studies which raises concerns over misdiagnosis.
Authors: Joaquim J. Ferreira, M.D., Ph.D., Faculdade de Medicina da Universidade de Lisboa, Lisbon, Portugal, and coauthors.
(doi:10.1001/jamaneurol.2019.3446)
Editor’s Note: The article includes conflict of interest disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Premature Death From Cardiovascular Disease
JAMA Cardiology
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 16, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamacardiology/fullarticle/10.1001/jamacardio.2019.3891?guestAccessKey=66b100a3-51c2-4b85-b8e3-0040bfe64230&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101619
What The Study Did: National data were used to examine changes from 2000 to 2015 in premature death (ages 25 to 64) from cardiovascular disease in the United States.
Authors: Yingxi Chen, M.D., Ph.D., of the National Cancer Institute in Rockville, Maryland, is the corresponding author.
(doi:10.1001/jamacardio.2019.3891)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Breastfeeding Disparities Among US Children by Race/Ethnicity
JAMA Pediatrics
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 14, 2019
Media advisory: To contact corresponding author Ruowei Li, M.D., Ph.D., email Anita Blankenship at aob4@cdc.gov. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamapediatrics/fullarticle/10.1001/jamapediatrics.2019.3319?guestAccessKey=2eb9dc6c-20eb-4c3c-9e68-51b646d3ac48&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101419
Bottom Line: Overall rates of breastfeeding increased from 2009 to 2015 but they varied by race/ethnicity in this observational study that used national survey data for nearly 168,000 infants in the United States. When breastfeeding rates took into account sociodemographic factors, such as participation in the Special Supplemental Nutrition Program for Women, Infants and Children, marital status, maternal education level and household income, the breastfeeding disparities were larger between black and white infants. For example, the difference for exclusive breastfeeding through six months increased from 0.5 to 4.5 percentage points. Breastfeeding differences between infants from all other nonwhite groups (Hispanic, Asian and American Indian or Alaskan Native) and white infants mostly got smaller or stayed the same, largely because of breastfeeding increases among white infants. All breastfeeding rates (ever, exclusive through six months, and continuation at 12 months) were lower for black infants than white infants in 2014-2015. Limitations of the study include the data from a national survey that excluded households without telephones. Efforts to improve breastfeeding rates among black infants are needed.
Authors: Ruowei Li, M.D., Ph.D., of the Centers for Disease Control and Prevention, Atlanta, and coauthors
(doi:10.1001/jamapediatrics.2019.3319)
Editor’s Note: Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Visual abstract, link to provide your readers free access to the full-text article
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), FRIDAY, OCTOBER 11, 2019
Want to embed a link to this study in your story? This full-text link will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.13054?utm_source=JAMA_Network&utm_medium=referral&utm_campaign=ftm_links&utm_term=101119
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
Visual Abstract

(doi:10.1001/jamanetworkopen.2019.13054)
Editor’s Note: The article contains funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamaneurology/fullarticle/10.1001/jamaneurol.2019.3403?guestAccessKey=b1769b38-7871-4767-86f9-8e6afa4ceef7&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101419
Emerging Increase in Electronic Cigarette Use by Young Adults between 2017-2018
JAMA Internal Medicine
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 14, 2019
Media advisory: To contact corresponding author Wei Bao, M.D., Ph.D., email Tom Snee at Tom-snee@uiowa.edu. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/10.1001/jamainternmed.2019.4957?guestAccessKey=5f47d068-7a56-422f-b0b6-1656d98ff144&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101419
Bottom Line: This research letter uses updated national survey data for 2018 to estimate how common electronic cigarette use is among adults 18 and older in the United States. The analysis included about 153,000 survey participants, of whom 55% were women. The authors report that while current e-cigarette use decreased from 3.7% in 2014 to 2.8% in 2017, it increased again in 2018 to 3.2%. The biggest increase between 2017-2018 was among young adults aged 18 to 24 years (5.2% in 2017 vs. 7.6% in 2018), with no such increase among middle-age or older adults. Limitations of the study include self-reported e-cigarette use. The authors stress their findings are of public health concern and that interventions to decrease e-cigarette use among young adults are needed.
Authors: Wei Bao, M.D., Ph.D., of the University of Iowa, Iowa City, and coauthors
(doi:10.1001/jamainternmed.2019.4957)
Editor’s Note: Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Association Between Weight-Loss Surgery in Women and Risk of Birth Defects in Infants
JAMA
EMBARGOED FOR RELEASE: 11 A.M. (ET), TUESDAY, OCTOBER 15, 2019
Media advisory: To contact corresponding author Martin Neovius, Ph.D., email martin.neovius@ki.se. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.12925?guestAccessKey=27aad08c-4798-435b-a157-e1fe0db8b554&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101419
Bottom Line: Researchers used national registry data in Sweden to examine the risk of major birth defects in infants born to women who had gastric bypass surgery compared with infants born to women who didn’t have the surgery but were similar based on other factors including maternal body mass index and diabetes. The analysis included 2,921 women who had Roux-en-Y gastric bypass surgery and 30,573 women who didn’t for comparison. Infants born to women who had gastric bypass surgery had lower risk of major birth defects. Study authors speculate that surgery-induced improvements in glucose control and other benefits associated with weight loss may contribute to reducing the risk of major birth defects. Limitations of the study include pregnancy termination data that was unavailable, not including stillbirths and individual birth defects couldn’t be analyzed.
Authors: Martin Neovius, Ph.D., Karolinska Institutet, Stockholm, Sweden, and coauthors.
(doi:10.1001/jama.2019.12925)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Clinical Trial Tests Varenicline to Help Adolescents, Young Adults Quit Smoking
JAMA Pediatrics
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 14, 2019
Media advisory: To contact corresponding author Kevin M. Gray, M.D., email Montez Seabrook at seabromo@musc.edu. The full study and editorial are linked to this news release.
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamapediatrics/fullarticle/10.1001/jamapediatrics.2019.3553?guestAccessKey=9ac5aef0-6ea0-46d4-ad11-501bd8e908e4&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101419
Bottom Line: Many adult cigarette smokers start before they turn 21 and this randomized clinical trial of volunteer participants tested how effective the smoking-cessation medication varenicline was in helping adolescents and young adults to quit. The 157 volunteers seeking treatment to quit ranged in age from 14 to 21; 77 participants received a 12-week course of varenicline and 80 received placebo but both groups received weekly smoking cessation counseling. The authors report the medicine was well tolerated but abstinence rates at the end of treatment, which was the trial’s primary outcome, didn’t differ between the two groups. However, secondary findings suggest varenicline helped smokers achieve self-reported abstinence earlier and better self-reported overall abstinence during treatment and at posttreatment follow-up. A potential limitation of the study was that biomarkers used to verify smoking abstinence may have been affected by participants who used marijuana or electronic cigarettes.
Authors: Kevin M. Gray, M.D., Medical University of South Carolina, Charleston, and coauthors
(doi:10.1001/jamapediatrics.2019.3553)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.13249?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=101119
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.13123?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=101119
Barriers to Access to Hearing Aids for Children
JAMA Otolaryngology-Head & Neck Surgery
EMBARGOED FOR RELEASE: 11 A.M. (ET), THURSDAY, OCTOBER 10, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamaotolaryngology/fullarticle/10.1001/jamaoto.2019.2877?guestAccessKey=c1a8b984-4097-4680-9c4c-0d582eb03643&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101019
What The Study Did: Researchers looked at demographic, socioeconomic and clinical factors that were associated with timely access to hearing aids for children.
Authors: Jonathan Walsh, M.D., of the Johns Hopkins University School of Medicine in Baltimore, is the corresponding author.
(doi:10.1001/jamaoto.2019.2877)
Editor’s Note: Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Firearm-Related Eye Injuries to Patients Under 21
JAMA Ophthalmology
EMBARGOED FOR RELEASE: 11 A.M. (ET), THURSDAY, OCTOBER 10, 2019
Media advisory: To contact corresponding author Joyce N. Mbekeani, M.D., F.R.C.S., F.R.C.Ophth., email Rachael McCallen at RMCCALL@montefiore.org. The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamaophthalmology/fullarticle/10.1001/jamaophthalmol.2019.3562?guestAccessKey=6e4372e4-f2c7-4461-950c-17eac3009125&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=101019
Bottom Line: Researchers used data from a national registry of hospitalized trauma cases in the United States to examine patterns of firearm-related eye injuries among patients under age 21 from 2008 through 2014. There were about 8,700 eye injuries from firearms in the U.S. during that time, of which nearly a quarter (1,972) were in patients under 21, mostly male adolescents ages 12 to 18. Black patients were most likely to be injured in assaults and white patients were most likely to have self-inflicted firearm-related eye injuries. Most firearm-related eye injuries were sight-threatening and associated with severe injury and traumatic brain injury. About 12% of patients died from their injuries in the hospital. Limitations of this observational study include the exclusion of patients who weren’t hospitalized because they died at the scene, which may underestimate the true implications of firearm-related eye trauma.
Authors: Joyce N. Mbekeani, M.D., F.R.C.S., F.R.C.Ophth., Montefiore Medical Center, Bronx, New York, and coauthors.
(doi:10.1001/jamaophthalmol.2019.3562)
Editor’s Note: Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Study Assesses Cost of Overpayments for Topical Prescription Medications
JAMA Dermatology
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 9, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamadermatology/fullarticle/10.1001/jamadermatol.2019.3078?guestAccessKey=c5c178d0-6aee-4ff5-9256-81da7592f27a&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100919
What The Study Did: This study examined how common and at what cost is the practice of so-called “clawbacks” for topical prescription drugs when an insured patient’s copayment exceeds the insurer’s cost for the drug.
Authors: Joslyn Kirby, M.D., M.S., M.Ed., of the Penn State Milton S. Hershey Medical Center in Hershey, Pennsylvania, is the corresponding author.
(doi:10.1001/jamadermatol.2019.3078)
Editor’s Note: Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Long-Term Outcomes for Transplant Patients Who Receive High-Risk Donor Lungs
JAMA Surgery
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 9, 2019
Media advisory: The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamasurgery/fullarticle/10.1001/jamasurg.2019.4079?guestAccessKey=9110ee31-f9bc-4a68-8dca-356015ca3622&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=1000919
What The Study Did: Researchers compared long-term outcomes between transplant patients who received conventional donor lungs and those who received high-risk donor lungs that had been assessed and reconditioned outside the body through a technique known as ex vivo lung perfusion.
Authors: Jussi M. Tikkanen, M.D., of Toronto General Hospital in Toronto, is the corresponding author.
(doi:10.1001/jamasurg.2019.4079)
Editor’s Note: The article includes conflict of interest disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Differences in Severity, Health Care Utilization for Firearm Injuries, Other Penetrating Trauma in Kids
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 9, 2019
Media advisory: To contact corresponding author Ashley E. Wolf, M.D., email press@seattlechildrens.org. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.12850?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=100919
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
Bottom Line: Pediatric firearm injuries were associated with greater severity and health care utilization than other penetrating trauma suffered by children caused by cutting or piercing, such as with a knife. This observational study used national trauma data in the United States from 2007 through 2016 to analyze 25,155 hospital encounters for firearm injury and 21,270 encounters for a cut or pierce injury in children 17 years old or younger. Firearm injuries were more likely to require admission to the intensive care unit (ICU) and have a higher degree of severity, as well as longer hospital and ICU stays, compared to cut or pierce injuries. Bullets have more force than many other weapons used to inflict a cut or pierce injury. Limitations of the study include that the data aren’t fully comprehensive. Study authors suggest pediatric firearm injuries can be reduced through legislative efforts, safe gun storage practices and community-based interventions.
Authors: Ashley E. Wolf, M.D., formerly of Seattle Children’s Hospital, University of Washington, Seattle, but now at Rush University Medical Center, Chicago, and coauthors
(doi:10.1001/jamanetworkopen.2019.12850)
Editor’s Note: The article includes conflict of interest disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.12895?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=100919
Elevated Risk of Blood Clot in Lungs After Surgery Lasts for How Long?
JAMA Surgery
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 9, 2019
Media advisory: The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamasurgery/fullarticle/10.1001/jamasurg.2019.3742?guestAccessKey=03a95875-89ab-4962-88d0-2dc65e687255&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100919
What The Study Did: Researchers examined how long an increased risk of pulmonary embolism (lung artery blockage usually caused by a blood clot) persisted after six types of surgery (vascular, gynecological, gastrointestinal, hip or knee replacement, fractures and other orthopedic operations) among 60,000 cancer-free middle-age adults using data from a French national inpatient database.
Authors: Alexandre Caron, M.D., of the University Lille in France, is the corresponding author.
(doi:10.1001/jamasurg.2019.3742)
Editor’s Note: The article includes funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Large Income Change Associated With Cardiovascular Disease Risk
JAMA Cardiology
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 9, 2019
Media advisory: To contact corresponding author Scott D. Solomon, M.D., email Elaine St. Peter at estpeter@bwh.harvard.edu. The full study, commentary and podcast are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamacardiology/fullarticle/10.1001/jamacardio.2019.3788?guestAccessKey=934dce44-ce9b-4bfe-9e47-01415e543e3b&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100919
Bottom Line: Whether a significant change in income is associated with risk of cardiovascular disease (CVD) was the focus of this observational study. Previous research has indicated that having a higher income is associated with lower risk of CVD; however, there is limited evidence on the association between changes in income and CVD. Using data from the ongoing Atherosclerosis Risk in Communities study, this analysis included nearly 9,000 participants from four areas of the United States (Jackson, Mississippi; Washington County, Maryland; suburbs of Minneapolis; and Forsyth County, North Carolina) who were categorized based on changes in their reported income. A drop in income of 50% or more was associated with higher risk of CVD (including heart attack, fatal coronary heart disease, heart failure or stroke) during an average follow-up of 17 years, while a 50% or more increase in income was associated with lower risk of CVD. A limitation of the study is the possibility that participants who developed health issues may have been more likely to experience a decrease in income.
Authors: Scott D. Solomon, M.D., Brigham and Women’s Hospital, Harvard Medical School, Boston, and coauthors.
(doi:10.1001/jamacardio.2019.3788)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.13051?guestAccessKey=b6f00aa9-8927-457e-9e19-d7bb983256ad&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=1008919
Retraction and Republication
JAMA
EMBARGOED FOR RELEASE: 11 A.M. (ET), TUESDAY, OCTOBER 8, 2019
Media advisory: The related articles are linked.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.10943?guestAccessKey=0c8e7495-72ba-4c4a-bf11-2992d40affc1&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100819
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations
Association of Family Relationships During Adolescence With Later Depression Risk
JAMA Pediatrics
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 7, 2019
Media advisory: To contact authors Ping Chen, Ph.D., and Kathleen Mullan Harris, Ph.D., email Melody Kramer at mjkramer@email.unc.edu. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamapediatrics/fullarticle/10.1001/jamapediatrics.2019.3336?guestAccessKey=c370ed0c-0fdd-4dd2-ab08-984022018fa0&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100719
Bottom Line: Positive family relationships during adolescence appeared to be associated with lower levels of depressive symptoms from adolescence to midlife in this observational study of about 18,000 adolescents followed up until they were 32 to 42 years old. The study examined differences between males and females in depressive symptoms by levels of positive family relationships during adolescence as measured by family cohesion (adolescent reports about how much their family understood them, had fun, and paid attention to them) and the absence of parent-child conflict (adolescent reports of a serious argument in the past month over their behavior). Family cohesion and the absence of parent-child conflict were associated with a lower risk of depression from adolescence into midlife. The reduction in depressive symptoms associated with positive adolescent family relationships was greater for females than males during adolescence and into the early 20s but then leveled out to be equally beneficial for males and females throughout young adulthood into midlife. Limitations of the study include a self-reported measure of depressive symptoms and preadolescent family relationships weren’t examined.
Authors: Ping Chen, Ph.D., and Kathleen Mullan Harris, Ph.D., of the Carolina Population Center at the University of North Carolina at Chapel Hill
(doi:10.1001/jamapediatrics.2019.3336)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
How Common is High Blood Pressure Among Children Worldwide?
JAMA Pediatrics
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 7, 2019
Media advisory: To contact corresponding author Yajie Zhu, Ph.D., email yajie.zhu@georgeinstitute.ox.ac.uk. The full study and editorial are linked to this news release.
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamapediatrics/fullarticle/10.1001/jamapediatrics.2019.3310?guestAccessKey=74d63283-8af6-41a6-9444-7b314482badc&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100719
Bottom Line: This study, called a review and meta-analysis, combined the results of 47 articles published from 1994 to 2018 to estimate worldwide how common high blood pressure is among children and adolescents age 19 and younger. Authors report the overall proportion of childhood hypertension was 4%. Hypertension was more common among overweight or obese children and those undergoing puberty. How common hypertension was also varied when measured by different devices. A limitation of this analysis was variation in reported prevalence among included studies. The findings suggest childhood high blood pressure is a considerable public health challenge worldwide.
Authors: Yajie Zhu, Ph.D., University of Oxford, United Kingdom, and coauthors
(doi:10.1001/jamapediatrics.2019.3310)
Editor’s Note: The article contains conflict of interest disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Did Providing Free Essential Medicines Increase Adherence?
JAMA Internal Medicine
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 7, 2019
Media advisory: To contact corresponding author Navindra Persaud, M.D., M.Sc., C.C.F.P., email Michael Oliveira at Michael.Oliveira@unityhealth.to. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/10.1001/jamainternmed.2019.4472?guestAccessKey=3a5a5e5e-1ccb-4562-b29c-ce6b1037ba3a&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100719
Bottom Line:More patients who said they couldn’t afford their medications adhered to treatment when they received free essential medicines for one year in a randomized clinical trial, but not all measures of health outcomes improved. The trial enrolled 786 patients (764 completed it) at nine primary care sites in Ontario, Canada. Patients were randomly split into two groups: 395 received free essential medicines plus usual care and 391 had usual care and usual access to medicines. Medicines aren’t universally publicly funded in Canada like hospitalizations and physician care are. Free medicines included in the trial were treatments for chronic conditions, such as antipsychotics, antiretrovirals, glucose-lowering medicines and antihypertensives, and for acute conditions, such as antibiotics and analgesics. Researchers report more people who received free essential medicines were appropriately adherent (151 of 395 or 38.2%) compared with those in the group with usual access to medicine (104 of 391 or 26.6%). The free distribution of medicine reduced systolic blood pressure among those prescribed an antihypertensive but it didn’t significantly improve low-density lipoprotein cholesterol levels and there was a nonsignificant improvement in diabetes control (decrease in hemoglobin A1c ) in those prescribed treatment to control diabetes. The importance of these findings from one high-income country should be applied cautiously to other locales with different health care systems.
Authors: Navindra Persaud, M.D., M.Sc., C.C.F.P., of St. Michael’s Hospital, Toronto, and coauthors
(doi:10.1001/jamainternmed.2019.4472)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.12443?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=100419
25% of Total US Health Care Spending Estimated to be Waste
JAMA
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, OCTOBER 7, 2019
Media advisory: To contact corresponding author William H. Shrank, M.D., M.S.H.S., email Alex Kepnes at akepnes@humana.com. The full study, editorials and podcast are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.13978?guestAccessKey=bf8f9802-be69-4224-a67f-42bf2c53e027&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100719
Bottom Line: A new study estimates about one-quarter of total health care spending in the United States is waste, with a price tag ranging from $760 billion to $935 billion. The United States spends more on health care than any other country. For this analysis, the authors identified government-based reports, articles and peer-reviewed publications from 2012 to 2019 that focused on estimates of costs or savings related to six areas of waste. There were 71 estimates from 54 publications and those estimates were combined into ranges or totaled. Study authors report total estimated annual cost of waste was $265.6 billion for administrative complexity (billing and coding waste, physician time spent reporting on quality measures); $230.7 billion to $240.5 billion for pricing failure (prices increase far from those expected in a well-functioning market); $102.4 billion to $165.7 billion for failure of care delivery (poor execution or lack of widespread adoption of best care processes); $75.7 billion to $101.2 billion for overtreatment or low-value care; $58.5 billion to $83.9 billion for fraud and abuse; and $27.2 billion to $78.2 billion for failure of care coordination (unnecessary admissions or avoidable complications and readmissions). The authors also searched the published literature to find estimates of the potential to reduce waste in each of the categories listed by scaling proven strategies. Projected potential savings from efforts to reduce waste ranged from $191 billion to $282 billion, a potential 25% reduction in the total cost of waste. The authors highlight the opportunity to reduce waste through insurer-clinician collaboration and data interoperability. This analysis has limitations, including that the studies used may not represent all costs and savings in each area of waste, and that data from some of the studies may not be generalizable to the U.S. population. Implementing effective measures to decrease waste is a chance to reduce continued increases in U.S. health care costs.
Authors: William H. Shrank, M.D., M.S.H.S., Humana Inc., Louisville, Kentucky, and coauthors
(doi:10.1001/jama.2019.13978)
Editor’s Note: The article includes conflict of interest disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email media relations.
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.12516?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=100419
Evaluating Value of Senses
JAMA Ophthalmology
EMBARGOED FOR RELEASE: 11 A.M. (ET), THURSDAY, OCTOBER 3, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamaophthalmology/fullarticle/10.1001/jamaophthalmol.2019.3537?guestAccessKey=1072c858-6c49-4033-875e-140f872c04d8&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100319
What The Study Did: What senses (sight, hearing, touch, smell, taste, balance, temperature and pain) are most valued by the general public? That’s the question this web-based survey in the U.K. answered.
Authors: David P. Crabb, Ph.D., of the University of London, is the corresponding author.
(doi:10.1001/jamaophthalmol.2019.3537)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Cost-Effectiveness of Multigene Testing of All Patients With Breast Cancer
JAMA Oncology
EMBARGOED FOR RELEASE: 11 A.M. (ET), THURSDAY, OCTOBER 3, 2019
Media advisory: The full study and podcast are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamaoncology/fullarticle/10.1001/jamaoncol.2019.3323?guestAccessKey=583f4614-cd6e-4be8-96a9-8db42b4763dd&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100319
What The Study Did: Researchers estimated the cost-effectiveness and health effects of multigene testing for all patients with breast cancer compared with selective testing based on family history or clinical criteria using data for nearly 12,000 women with breast cancer from the U.S., U.K. and Australia.
Authors: Ranjit Manchanda, M.D., Ph.D., of the Queen Mary University of London, is the corresponding author.
(doi:10.1001/jamaoncol.2019.3323)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Changes Over Time in Cases of Head/Neck Melanoma Among Kids, Teens, Young People in US, Canada
JAMA Otolaryngology-Head & Neck Surgery
EMBARGOED FOR RELEASE: 11 A.M. (ET), THURSDAY, OCTOBER 3, 2019
Media advisory: The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamaotolaryngology/fullarticle/10.1001/jamaoto.2019.2769?guestAccessKey=9bfdcb86-2790-47ba-b577-bdc9896ba33b&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100319
What The Study Did: This observational study looked at changes in new cases of head and neck melanoma among children, adolescents and young adults in the U.S. and Canada over a 20-year period from 1995 to 2014.
Authors: Haley N. Bray, M.D., of the Saint Louis University School of Medicine in Missouri, is the corresponding author.
(doi:10.1001/jamaoto.2019.2769)
Editor’s Note: Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.12352?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=100219
Here’s a link to provide your readers free access to the full-text article
Media advisory: This article is being released to coincide with presentation at the European Society of Intensive Care Medicine (ESICM) annual congress in Berlin.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.14608?guestAccessKey=97c21250-7922-4a3b-8086-1b4f0eee6ec8&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100219
Here’s a link to provide your readers free access to the full-text article
Media advisory: This article is being released to coincide with presentation at the European Society of Intensive Care Medicine (ESICM) annual congress in Berlin.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.14901?guestAccessKey=3a37cddc-c94a-4ce2-91c4-3043ae779131&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100219
Here’s a link to provide your readers free access to the full-text article
Media advisory: This article is being released to coincide with presentation at the European Society of Intensive Care Medicine (ESICM) annual congress in Berlin.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.14607?guestAccessKey=7c75fd20-5e1f-47d2-9bc7-ec47375fc7e1&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100219
Going to Sleep on Your Back in Late Pregnancy
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 2, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.12614?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=100219
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
What The Study Did: This study looked at whether going to sleep on your back in the third trimester of pregnancy was associated with average lower birth weights.
Authors: Lesley M.E. McCowan, M.D., of the University of Auckland in New Zealand, is the corresponding author.
(doi:10.1001/jamanetworkopen.2019.12614)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Maternal Lead Exposure, Intergenerational Risk of Childhood Overweight/Obesity and Folate
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 2, 2019
Media advisory: The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.12343?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=100219
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
What The Study Did: An observational study of 1,442 mother-child pairs examined associations between lead blood levels in mothers and intergenerational risk of their children being overweight or obese and whether adequate folate levels in mothers mitigated that risk.
Authors: Xiaobin Wang, M.D., M.P.H., Sc.D., of the Johns Hopkins Bloomberg School of Public Health in Baltimore, is the corresponding author.
(doi:10.1001/jamanetworkopen.2019.12343)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Grading Evidence in Studies About Antidepressant Use/Exposure and Adverse Health Outcomes
JAMA Psychiatry
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 2, 2019
Media advisory: The full study and editorial are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamapsychiatry/fullarticle/10.1001/jamapsychiatry.2019.2859?guestAccessKey=5481e8d7-21f2-4ed3-8aad-9e3ab14a3225&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100219
What The Study Did: This study graded the evidence of 45 meta-analyses of observational studies on the association between antidepressant use or exposure and adverse health outcomes.
Authors: Elena Dragioti, Ph.D., of Linköping University in Linköping, Sweden, is the corresponding author.
(doi:10.1001/jamapsychiatry.2019.2859)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetw
ADHD and Risk of Giving Birth as Teenagers
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 2, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.12463?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=100219
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
What The Study Did: Data were used from about 384,000 girls and women in Sweden (including 6,410 with attention-deficit/hyperactivity disorder) who gave birth for the first time between 2007-2014 to examine whether those with ADHD have an increased likelihood of giving birth as teenagers.
Authors: Charlotte Skoglund, Ph.D., of the Karolinska Institute in Stockholm, is the corresponding author.
(doi:10.1001/jamanetworkopen.2019.12463)
Editor’s Note: The article contains funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Lifetime Indoor Tanning Associated With Squamous Cell Carcinoma Cancer
JAMA Dermatology
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 2, 2019
Media advisory: The full study and editorial are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamadermatology/fullarticle/10.1001/jamadermatol.2019.2681?guestAccessKey=16542ca9-1c94-4522-86fa-3989d6b8061d&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=100219
What The Study Did: This observational study used data from nearly 160,000 women in Norway to examine lifetime indoor tanning and risk of squamous cell carcinoma, one of the most common types of cancer worldwide. The findings suggest the association between cumulative exposure to indoor tanning and risk of squamous cell carcinoma was the same regardless of how many years the women tanned and what age they were when they started.
Authors: Simon Lergenmuller, M.Sc., of the University of Oslo, Norway, is the corresponding author.
(doi:10.1001/jamadermatol.2019.2681)
Editor’s Note: The article contains funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Earnings Disparities Between Female, Male Surgeons in Canada
JAMA Surgery
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 2, 2019
Media advisory: To contact corresponding author Nancy N. Baxter, M.D., Ph.D., email Jennifer Stranges at Jennifer.Stranges@unityhealth.to. The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamasurgery/fullarticle/10.1001/jamasurg.2019.3769?guestAccessKey=ca5dfc05-a79c-4c66-8546-7512c3452071&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100219
Bottom Line: Female surgeons in Ontario, Canada, earned less per hour than their male counterparts within a fee-for-service system, and women were less likely to perform the most lucrative procedures. Fee-for-services systems of payment are often proposed as being unbiased. This analysis used administrative data from a single-payer health system to compare earnings per hour spent operating for 3,275 surgeons who performed 1.5 million surgical procedures between 2014 and 2016. Female surgeons had practiced fewer years than male surgeons and the largest proportion of female surgeons practiced gynecology. Researchers report female surgeons earned 24% less per hour than male surgeons, with the largest average earning differences in cardiothoracic surgery at nearly $60 (in US dollars) per hour and orthopedic surgery at $55 per hour. Limitations of the study include the small number of women in some specialties, limiting the ability to identify earnings differences. Earnings differences also may have been underestimated.
Authors: Nancy N. Baxter, M.D., Ph.D., University of Toronto, Ontario, Canada, and coauthors
(doi:10.1001/jamasurg.2019.3769)
Editor’s Note: The article includes funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations
Here’s a link to provide your readers free access to the full-text article
Media advisory: This article is being released to coincide with the opening of the European Society for Medical Oncology (ESMO) Congress 2019 in Barcelona, Spain.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamaoncology/fullarticle/10.1001/jamaoncol.2019.2996?guestAccessKey=e077cbf5-5a57-4ace-b5cc-edff3cf74311&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=092719
Here’s a link to provide your readers free access to the full-text article
Media advisory: This article is being released to coincide with presentation at the European Society for Medical Oncology (ESMO) Congress 2019 in Barcelona, Spain.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamaoncology/fullarticle/10.1001/jamaoncol.2019.4794?guestAccessKey=6bddf612-f517-465c-bbf3-5f5b5061f57b&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=093019
Here’s a link to provide your readers free access to the full-text article
Media advisory: This article is being released to coincide with presentation at the European Society for Medical Oncology (ESMO) Congress 2019 in Barcelona, Spain.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamaoncology/fullarticle/10.1001/jamaoncol.2019.4782?guestAccessKey=570a7e0e-e643-4edf-99c0-37fa07fa32b9&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=092919
How Were Oral Contraceptives, Concurrent Depressive Symptoms Associated Among Adolescents, Young Women?
JAMA Psychiatry
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, OCTOBER 2, 2019
Media advisory: To contact corresponding author Anouk E. de Wit, B.Sc., email a.e.de.wit@umcg.nl. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamapsychiatry/fullarticle/10.1001/jamapsychiatry.2019.2838?guestAccessKey=653456f6-38a8-4a18-8150-dd9cbcf099a3&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100219
Bottom Line: This observational study examined associations between depressive symptoms and oral contraceptive use in adolescents and young women and how those associations might differ by age. Oral contraceptive use has been associated with increased risk for subsequent depression in adolescents. The study included about 1,000 girls and young women in the Netherlands who completed at least 1 of 4 assessments about their oral contraceptive use and depressive symptoms at ages 16, 19, 22 and 25. Authors report oral contraceptive use showed no association with depressive symptoms when all the age groups were combined. However, 16-year-old girls who used oral contraceptives reported higher depressive symptoms scores and were more likely to report crying, eating problems and excessive sleepiness than those who didn’t use oral contraceptives. Limitations of the study include causal inferences cannot be made, and the results may not be generalizable to other countries where access to contraception and the acceptability of its use are different.
Authors: Anouk E. de Wit, B.Sc., University of Groningen, the Netherlands, and coauthors.
(doi:10.1001/jamapsychiatry.2019.2838)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
How Common is Food Insecurity Among Medicare Enrollees?
JAMA Internal Medicine
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, SEPTEMBER 30, 2019
Media advisory: To contact corresponding author Jeanne M. Madden, Ph.D., email Shannon Nargi at s.nargi@northeastern.edu. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/10.1001/jamainternmed.2019.3900?guestAccessKey=b80b24f0-2baf-413a-9b72-2e7a71ed2ab3&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=093019
Bottom Line: Nearly 1 in 10 Medicare enrollees age 65 and over and 4 in 10 enrollees younger than 65 with long-term disabilities experience food insecurity. This study provides national estimates of how common it is for Medicare enrollees to be unable to get the food they need because they lack money. Study authors used data from a 2016 survey of Medicare beneficiaries with six questions about food insecurity. The nearly 9,700 people interviewed represented 50.7 million Medicare enrollees living in community settings. Analysis of risk factors found that lower incomes, reporting four or more chronic condition diagnoses, and having symptoms of depression or anxiety were each independently associated with food insecurity in both age groups. A limitation of this observational study is that it cannot determine causality.
Authors: Jeanne M. Madden, Ph.D., of Northeastern University, Boston, and coauthors
(doi:10.1001/jamainternmed.2019.3900)
Editor’s Note: The article includes funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamapediatrics/fullarticle/10.1001/jamapediatrics.2019.3480?guestAccessKey=082e517a-8472-4c89-bceb-d3c2f3b72352&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=093019
Rural, Urban Drive Times to Nearest Opioid Treatment Programs Differ
JAMA
EMBARGOED FOR RELEASE: 11 A.M. (ET), TUESDAY, OCTOBER 1, 2019
Media advisory: To contact corresponding author Paul J. Joudrey, M.D., M.P.H., email Bill Hathaway at william.hathaway@yale.edu. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.12562?guestAccessKey=3b2b2fb6-9390-43c0-9437-86057c608fcd&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100119
Bottom Line: Comparing drive times to the nearest opioid treatment programs in urban and rural counties in five U.S. states with the highest county rates of opioid-related overdose deaths was the focus of this research letter. Methadone for treating opioid use can only be dispensed from certified treatment programs in the United States, of which there is a shortage in rural counties. This analysis included 489 counties in Indiana, Kentucky, Ohio, Virginia and West Virginia. Among all the counties, average drive time to the nearest opioid treatment programs was 37 minutes. Longer drive times were associated with rural counties compared with urban ones, with driving times ranging from 41 to 49 minutes in rural counties compared with eight to 35 minutes in urban counties. Longer drive times in the most rural counties could be reduced from 49 minutes to 17 minutes if methadone prescribing occurred at federally qualified health centers (federally supported primary care clinics). Limitations of the study include drive times were county-level population estimates, individual drive times within counties vary, and the geographic availability of methadone in urban areas was likely overestimated because of public transportation.
Authors: Paul J. Joudrey, M.D., M.P.H., Yale School of Medicine, New Haven, Connecticut, and coauthors
(doi:10.1001/jama.2019.12562)
Editor’s Note: The article includes funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations
Prior DUI Convictions Among Legal Handgun Purchasers Associated With Risk of Later Violent Crimes
JAMA Internal Medicine
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, SEPTEMBER 30, 2019
Media advisory: To contact corresponding author Rose M.C. Kagawa, Ph.D., M.P.H., email Carole Gan at cfgan@ucdavis.edu. The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/10.1001/jamainternmed.2019.4491?guestAccessKey=2e65dc76-96cc-43c5-a5c7-33ddf3e34108&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=093019
Bottom Line: A study of legal handgun purchasers in California suggests convictions for driving under the influence (DUI) prior to a gun purchase may be associated with subsequent risk of arrest for violent crimes, including firearm-related ones. The observational study included about 79,000 gun purchasers followed-up from their first gun purchase in 2001 through 2013. Of the 1,495 purchasers with DUI convictions, 131 (8.8%) were subsequently arrested for violent crimes listed on the Crime Index (murder, rape, robbery and aggravated assault) published by the FBI. Among 65,700 purchasers with no prior criminal history, 1,188 (1.8%) were subsequently arrested for Crime Index-listed violent crimes. Compared with gun purchasers who had no prior criminal history, gun purchasers with prior DUI convictions and no other criminal history were at increased risk of arrest for a Crime Index-listed violent crime, a firearm-related violent crime and any violent crime. Limitations of the study include the exclusion of gun purchasers age 50 and older thus limiting the generalizability of the findings. The federal government and many states have restricted the purchase and possession of firearms by members of high-risk groups, such as people convicted of felonies, domestic violence and other violent misdemeanors, and study authors suggest that similar restrictions on people convicted of DUI may help to reduce violent criminal activity.
Authors: Rose M.C. Kagawa, Ph.D., M.P.H., of the University of California, Davis, in Sacramento, and coauthors
(doi:10.1001/jamainternmed.2019.4491)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Did IV High-Dose Vitamin C Improve Outcomes for Patients With Sepsis and Severe Lung Condition?
JAMA
EMBARGOED FOR RELEASE: 11 A.M. (ET), TUESDAY, OCTOBER 1, 2019
Media advisory: To contact corresponding author Alpha A. Fowler III, M.D., email Laura Rossacher at lrossacher@vcu.edu. The full study and editorial are linked to this news release. A visual abstract is below.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jama/fullarticle/10.1001/jama.2019.11825?guestAccessKey=62db20f8-8ba0-4199-8a8c-de3b07be8551&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=100119
Bottom Line: This randomized clinical trial looked at whether high-dose vitamin C delivered intravenously could reduce organ failure, inflammation and vascular injury in patients with sepsis and acute respiratory distress syndrome (ARDS), a severe lung condition that is a common organ injury associated with sepsis. Previous research has suggested that intravenous vitamin C may lessen inflammation and vascular injury. In this trial, 167 patients with sepsis and ARDS at seven intensive care units in the United States received intravenous vitamin C or placebo every six hours for 96 hours. The authors report that compared with placebo, intravenous vitamin C didn’t result in improved measures of organ dysfunction or levels of biomarkers indicating inflammation (C-reactive protein) or vascular injury (the anticoagulant thrombomodulin) by seven days. Limitations of this preliminary study include that it may have been underpowered to detect differences in measures of organ failure and biomarker levels and the dosage of vitamin C may have been insufficient.
Authors: Alpha A. Fowler III, M.D., Virginia Commonwealth University, Richmond, and coauthors
Visual Abstract

(doi:10.1001/jama.2019.11825)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamaophthalmology/fullarticle/10.1001/jamaophthalmol.2019.3731?guestAccessKey=a193ec13-097b-4c55-9620-afed5b8edc82&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=092619
Optimism Associated With Lower Risk of Heart Disease, Early Death
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), FRIDAY, SEPTEMBER 27, 2019
Media advisory: To contact corresponding author Alan Rozanski, M.D., email Ilana Nikravesh at ilana.nikravesh@mountsinai.org. The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.12200?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=092719
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
Bottom Line: Optimism was associated with lower risk of cardiovascular events and less risk of overall death in this observational study. The study, called a systematic review and meta-analysis, combined results from 15 studies (10 studies reported data on cardiovascular events and nine reported data on all-cause mortality) with nearly 230,000 participants and an average follow-up of nearly 14 years. Limitations of the study include wide variation in ages of the participants; the inability to account for individual mitigating factors such as smoking, diabetes and hypertension; and a study design that doesn’t permit causal inferences to be made. Future studies should examine what might explain this association, as well as investigate the potential benefits of interventions that could promote optimism and reduce pessimism.
Authors: Alan Rozanski, M.D., Mount Sinai St. Luke’s Hospital, New York, and coauthors
(doi:10.1001/jamanetworkopen.2019.12200)
Editor’s Note: Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Smoking Cessation Program for Patients With, Without Cancer
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), FRIDAY, SEPTEMBER 27, 2019
Media advisory: To contact corresponding author Paul Cinciripini, Ph.D., email Meagan Raeke at meraeke@mdanderson.org. The full study and commentary are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.12251?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=092719
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
Bottom Line: A tobacco treatment program delivered at a cancer center had average seven-day smoking abstinence rates of about 45% at three- and six-month follow-ups and nearly 44% at the nine-month follow-up, and those rates didn’t differ between patients with and without cancer. This observational study included 3,245 participants in a model tobacco treatment program (2,343 with current cancer; 309 with a history of cancer; and 593 with no history of cancer) that consisted of an in-person medical consultation, in-person and telephone counseling sessions, and prescription drug therapy. Limitations of the study include that it wasn’t a randomized clinical trial. The findings suggest providing a comprehensive tobacco treatment program in an oncologic setting could foster smoking cessation, which can affect outcomes of patients with cancer who smoke.
Authors: Paul Cinciripini, Ph.D., the University of Texas MD Anderson Cancer Center, Houston, and coauthors
(doi:10.1001/jamanetworkopen.2019.12251)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Potential Factors Associated With Severity of Diabetes Complications in Patients With Mental Health, Substance Use Disorders
JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, SEPTEMBER 25, 2019
Media advisory: To contact corresponding author Eric M. Schmidt, Ph.D., email Kim Betton at Kim.Betton@va.gov. The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/10.1001/jamanetworkopen.2019.12060?utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_term=092519
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Wednesday and Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
Bottom Line: Among 123,000 patients in the U.S. Department of Veterans Affairs health system with newly diagnosed diabetes, 23% had mental health or substance use disorder diagnoses and that prior engagement with the health care system may be associated with a lower severity of complications for a few years after the onset of diabetes. More than 90% of patients with mental health or substance use disorders had primary care visits before diabetes was diagnosed compared with 58 percent of patients without those disorders. Patients with already diagnosed mental health and substance use disorders had lower overall, but more quickly progressing, complication severity scores through seven years after a diabetes diagnosis than those patients without, even after accounting for other mitigating factors such as coexisting illnesses. Study authors speculate patients with diagnosed mental health or substance use disorders likely were already being treated for other conditions, such as hypertension, when diabetes was diagnosed. Limitations of the study include missing data.
Authors: Eric Schmidt, Ph.D., Veterans Affairs Palo Alto Health Care System, Menlo Park, and Stanford University, Stanford, California, and coauthors
(doi:10.1001/jamanetworkopen.2019.112060)
Editor’s Note: The article contains funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Association of Genetic Risk to Psychotic Experiences With Neuropsychiatric Disorders
JAMA Psychiatry
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, SEPTEMBER 25, 2019
Media advisory: The full study and editorial are linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamapsychiatry/fullarticle/10.1001/jamapsychiatry.2019.2508?guestAccessKey=05958f32-6d33-4a01-8960-0ec0f4dba66b&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=092519
What The Study Did: Data from the UK Biobank were used to examine whether genetic risk to psychotic experiences is shared with neuropsychiatric disorders.
Authors: James T. R. Walters, M.R.C.Psych., Ph.D., and Stanley Zammit, M.R.C.Psych., Ph.D., of Cardiff University in Cardiff, United Kingdom, are the corresponding authors.
(doi:10.1001/jamapsychiatry.2019.2508)
Editor’s Note: The article includes conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Use of Mental Health Services After Weight-Loss Surgery
JAMA Psychiatry
EMBARGOED FOR RELEASE: 11 A.M. (ET), WEDNESDAY, SEPTEMBER 25, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time https://jamanetwork.com/journals/jamapsychiatry/fullarticle/10.1001/jamapsychiatry.2019.2741?guestAccessKey=13d2181c-aae0-4464-9062-d34c16e6be41&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=092519
What The Study Did: With data from nearly 25,000 patients who underwent weight-loss surgery in Western Australia over 10 years, this study examined the association between bariatric surgery and the use of outpatient, emergency department and inpatient mental health services.
Authors: David J.R. Morgan, M.B.B.S., St. John of God Subiaco Hospital, Perth, Western Australia, is the corresponding author.
(doi:10.1001/jamapsychiatry.2019.2741)
Editor’s Note: The article includes funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Changes in Internal Medicine Subspecialty Choices of Women, Men
JAMA Internal Medicine
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, SEPTEMBER 23, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/10.1001/jamainternmed.2019.3833?guestAccessKey=5eb41f98-9775-427e-ad39-586edac1e949&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=092319
What The Study Did: This study used enrollment data to examine changes in the internal medicine subspecialty choices of women and men from 1991 to 2016. Data were examined for nine internal medicine subspecialties: cardiovascular disease, endocrinology, gastroenterology, geriatric medicine, hematology and oncology, infectious disease, nephrology, pulmonary disease and critical care, and rheumatology.
Authors: Mary Norine Walsh, M.D., M.A.C.C., of the St. Vincent Hospital and Heart Center in Indianapolis, is the corresponding author.
(doi:10.1001/jamainternmed.2019.3833)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Use, Discontinuation of Insulin Treatment Among Older Adults
JAMA Internal Medicine
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, SEPTEMBER 23, 2019
Media advisory: The full study is linked to this news release.
Embed this link to provide your readers free access to the full-text article: This link will be live at the embargo time https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/10.1001/jamainternmed.2019.3759?guestAccessKey=e1982c2b-b1e4-48ef-b2ba-4b51e6e9b8f1&utm_source=For_The_Media&utm_medium=referral&utm_campaign=ftm_links&utm_content=tfl&utm_term=092319
What The Study Did: Whether insulin treatment was used less frequently and discontinued more often among older adults (ages 75 to 79) in poor health compared with those in good health was the focus of this observational study that included more than 21,000 adults with type 2 diabetes.
Authors: Jonathan Z. Weiner, M.D., M.P.H., of Kaiser Permanente of Northern California in Oakland, is the corresponding author.
(doi:10.1001/jamainternmed.2019.3759)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.
Here’s a link to provide your readers free access to the full-text article
Embed this link to provide your readers free access to the full-text article This link will be live at the embargo time: