JAMA Internal Medicine
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, JULY 16, 2018
Media advisory: To contact study author Katherine E. Fleming-Dutra, M.D., email Martha Sharan at msharan@cdc.gov. The full study is available on the For The Media website.
Want to embed a link to this study in your story? Links will be live at the embargo time https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/10.1001/jamainternmed.2018.1632
Translation available: A translation in simplified Chinese is available below.
本篇新闻发布稿件备有翻译版本:以下内容为中文简体翻译版本
Bottom Line: Outpatient antibiotic prescribing varied among traditional medical and retail clinic settings and during visits with respiratory diagnoses where antibiotics were inappropriate, patterns that suggest differences in patient mix and antibiotic overuse.
Why The Research Is Interesting: Antibiotic use contributes to antibiotic resistance, and antibiotic overuse is common, especially for viral respiratory infections. This study compared antibiotic prescribing patterns among urgent care centers, retail clinics, emergency departments and medical offices.
Who and When: Outpatient claims data from a 2014 database that captures claims data on people younger than 65 with employer-sponsored insurance
What (Measures and Outcomes): Outpatient claims at urgent care centers, retail clinics, hospital based-emergency departments or medical offices were each assigned a diagnosis (exposure); percentage of visits linked to prescription of antibiotics with a focus on respiratory diagnoses where antibiotics were unnecessary (outcomes)
How (Study Design): This was an observational study. Researchers were not intervening for purposes of the study and cannot control all the natural differences that could explain the study findings.
Authors: Katherine E. Fleming-Dutra, M.D., of the U.S. Centers for Disease Control and Prevention, Atlanta, Georgia, and coauthors
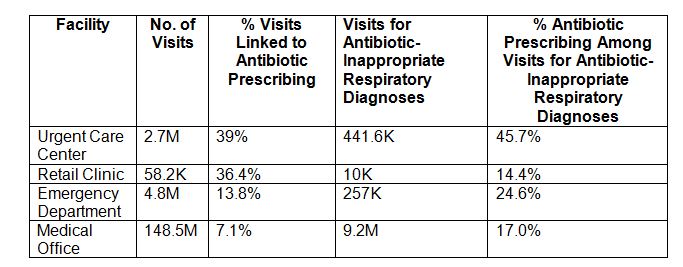
Results:
Study Limitations: Researchers could not clinically validate diagnoses in claims data so misclassification was possible, data also are not generalizable to populations not captured in this claims database, and facility codes could not be validated.
Study Conclusions: Antibiotic stewardship, the effort to optimize antibiotic use, across the spectrum of outpatient settings could help to improve antibiotic prescribing and patient care.
Related Material: The patient page, “I Have a Cold – What Do I Need to Know,” and the invited commentary, “Overprescription in Urgent Care Clinics – the Fast and the Spurious,” by JAMA Internal Medicine Editor Rita F. Redberg, M.D., M.Sc., of the University of California, San Francisco, and coauthors also are available on the For The Media website.
To Learn More: The full study is available on the For The Media website.
(doi:10.1001/jamainternmed.2018.1632)
Editor’s Note: The article contains funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or emailmediarelations@jamanetwork.org.
Translation in Simplified Chinese
中文简体翻译版本
禁止提前报道指令解除时间:2018年7月16日,星期一,美国东部时间上午11点
媒体咨询:联系研究作者Katherine E. Fleming-Dutra, M.D.,请发电子邮件到Martha Sharan msharan@cdc.gov。
传统与零售诊所在门诊抗生素处方上的比较
概要: 根据《美国医学会杂志-内科学》(JAMA Internal Medicine)发表的一项研究,传统和零售诊所在门诊抗生素处方上有所不同,而当有不适合使用抗生素的呼吸诊断的病人就诊时,不同类型的门诊在患者组成及抗生素过度使用等方面都有区别。
为何对该问题感兴趣:抗生素的使用可能会导致抗生素耐药性,而抗生素过度使用是很常见的,特别是对于病毒性呼吸道感染。 本研究比较了紧急护理中心,零售诊所,急诊室和医院门诊的抗生素处方模式。
研究参与者及时间:2014年数据库中的门诊索赔数据,该数据库记录了使用通过工作获得保险的65岁以下人群的索赔数据
研究内容(研究手段及结果):紧急护理中心,零售诊所,医院急诊室以及医院门诊的索赔均被分配一种诊断(暴露); 与抗生素处方相关的就诊百分比,并重点关注不需要抗生素的呼吸道诊断(结果)
如何研究(研究设计):这是一项观察性研究。 研究人员不会为研究目而进行干预,也无法控制可以解释研究结果的所有自然差异。
作者:Katherine E. Fleming-Dutra, M.D., 疾病预防与控制中心,佐治亚州亚特兰大, 以及共同作者
研究结果: 270万紧急护理中心就诊中的39.0%,58,206零售诊所就诊中的36.4%,480万急诊室就诊中的13.8%以及1亿485万医院门诊就诊中的7.1%与抗生素处方相关。
研究局限:研究人员无法临床验证索赔数据中的诊断,因此可能出现错误分类,数据也不能推广到未记录在此索赔数据库中的人群,并且无法验证各医疗设施代码。
研究结论:
在各个不同门诊类型中,抗生素管理,优化抗生素使用的努力可以帮助改善抗生素处方和患者护理。
欲了解更多信息:在下面网站可以获得该研究的全文,For The Media:https://media.jamanetwork.com/。