JAMA Network Open
EMBARGOED FOR RELEASE: 11 A.M. (ET), FRIDAY, MAY 18, 2018
Media advisory: To contact corresponding study author Christine M. Goertz, D.C., Ph.D., email James O’Connor at james.oconnor@palmer.edu. The full study is available on the For The Media website.
Want to embed a link to this study in your story? Links will be live at the embargo time https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2680417
About JAMA Network Open: JAMA Network Open is the new online-only open access general medical journal from the JAMA Network. Every Friday, the journal publishes peer-reviewed clinical research and commentary in more than 40 medical and health subject areas. Every article is free online from the day of publication.
Bottom Line: U.S military personnel with low back pain who received usual medical care plus chiropractic care reported moderate improvement in their pain intensity and disability compared with patients who received usual medical care alone.
Why The Research Is Interesting: Low back pain is one of the most common reasons service members in the U.S. military seek medical care. Common therapies for low back pain include nonsteroidal anti-inflammatory drugs, opioids, spinal fusions and edpidural steroid injections. An opioid crisis in the United States has created an urgent need to evaluate cost-effective and low-risk nonpharmacological treatments for low back pain. One of those options is chiropractic care.
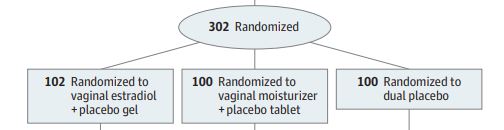
Who and When: 750 active-duty U.S. service members enrolled in a clinical trial at three military sites (250 at each site) conducted from September 2012 to February 2016
What (Study Interventions and Measures): Usual medical care (self-care, medications, physical therapy and pain clinic referral) or usual medical care plus chiropractic care (spinal manipulation in the low back and adjacent areas plus additional procedures such as rehabilitative exercise, cryotherapy, superficial heat and other manual therapies) over six weeks (interventions); low back pain intensity and disability scores (main outcomes)
How (Study Design): This was a clinical trial. Clinical trials allow for the strongest inferences to be made about the true effect of an intervention such as a medication or a procedure. However, not all clinical trial results can be replicated in real-world settings because patient characteristics or other variables may differ from those that were studied.
Authors: Christine M. Goertz, D.C., Ph.D., formerly of Palmer College of Chiropractic and now with Spine IQ (The Spine Institute for Quality), Davenport, Iowa, and coauthors
Results:
Study Limitations: Differences in participant characteristics, treatments received and outcomes across sites, as well as a short follow-up
Study Conclusions: Changes in pain intensity and disability reported by U.S. military personnel in this clinical trial that supports usual medical care plus chiropractic care for low back pain are consistent with existing literature on spinal manipulation therapy in both military and civilian populations.
Related Material: The invited commentary, “Innovating to Improve Care for Low Back Pain in the Military: Chiropractic Care Passes Muster,” by Daniel C. Cherkin, M.A., Ph.D., emeritus senior scientific investigator, Kaiser Permanente Washington Health Research Institute, Seattle, also is available on the For The Media website.
For more details and to read the full study, please visit the For The Media website.
(doi:10.1001/jamanetworkopen.2018.0105)
Editor’s Note: The article contains conflict of interest and funding support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or email mediarelations@jamanetwork.org.