JAMA Internal Medicine
EMBARGOED FOR RELEASE: 11 A.M. (ET), MONDAY, MARCH 19, 2018
Media advisory: To contact author Caroline M. Mitchell, M.D., email Julie Cunningham at Julie.cunningham@mgh.harvard.edu. The full study is available on the For The Media website.
Want to embed a link to this study in your story?: Links will be live at the embargo time https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/10.1001/jamainternmed.2018.0116
Translation available: A translation in simplified Chinese is available below.
Bottom Line: A prescribed vaginal estradiol hormone tablet and over-the-counter vaginal moisturizer didn’t provide more benefit than a placebo vaginal tablet and gel to reduce postmenopausal vulvovaginal symptoms in women.
Why The Research Is Interesting: Many postmenopausal women have bothersome vulvovaginal symptoms, including vaginal dryness, itching and pain with sex. Treatment recommendations for these symptoms focus mostly on vaginal products but issues with those treatments include messiness, expense, safety concerns and a lack of symptom relief. This study evaluated the efficacy of vaginal estradiol tablets and a vaginal moisturizer in women with moderate to severe vulvovaginal symptoms.
Who and When: 302 postmenopausal women with moderate to severe symptoms in a 12-week randomized clinical trial
What (Study Interventions and Measures):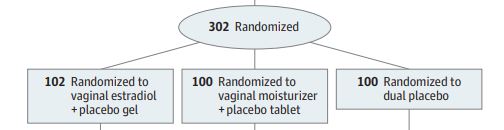
The main outcome was a decrease in the reported severity of symptoms.
How (Study Design): This was a randomized clinical trial (RCT). RCTs allow for the strongest inferences to be made about the true effect of an intervention. However, not all RCT results can be replicated in real-world settings because patient characteristics or other variables may differ from those studied in the RCT.
Authors: Caroline M. Mitchell, M.D., of Massachusetts General Hospital, Boston, and coauthors
Results: Vaginal estradiol tablets plus placebo gel and a vaginal moisturizer plus a placebo tablet were not better than dual placebo tablets and gel at reducing symptom severity or improving sexual function.
Study Limitations: The generalizability of study results is limited by the relatively homogeneous study population.
Study Conclusions: A better understanding of the underlying mechanism of postmenopausal vulvovaginal symptoms is needed to guide efforts to improve treatment options.
Related material: An author podcast and the invited commentary, “Rethinking the Approach to Managing Postmenopausal Vulvovaginal Symptoms,” by Alison J. Huang, M.D., M.A.S., M.Phil., of the University of California, San Francisco, and coauthors also are available on the For The Media website.
For more details and to read the full study, please visit the For The Media website.
(doi:10.1001/jamainternmed.2018.0116)
Editor’s Note: The article contains conflict of interest and funding/support disclosures. Please see the article for additional information, including other authors, author contributions and affiliations, financial disclosures, funding and support, etc.
# # #
For more information, contact JAMA Network Media Relations at 312-464-JAMA (5262) or emailmediarelations@jamanetwork.org.
Translation in Simplified Chinese
禁止提前报道指令解除时间:2018年3月19日,星期一,美国东部时间上午11点
媒体咨询:联系通讯作者Caroline M. Mitchell, M.D.,请发电子邮件到Julie Cunningham Julie.cunningham@mgh.harvard.edu。
对绝经后妇女外阴阴道症状的治疗
概要: 根据《美国医学会杂志 内科》(JAMA Internal Medicine)发表的一项研究称,处方药阴道雌二醇激素片剂和非处方药阴道保湿剂并不能比安慰剂阴道片剂和凝胶提供更多的益处来减少女性绝经后的外阴阴道症状。
为何对该问题感兴趣:许多绝经后妇女患有外阴阴道炎症状,包括阴道干涩,瘙痒和性交疼痛。 这些症状的治疗建议主要集中在一些阴道治疗产品,但这些治疗产品经常有一些问题, 如产品杂乱,费用高,安全问题和不能有效缓解症状等。 本研究评估了阴道雌二醇片剂和阴道保湿剂对中重度外阴阴道症状患者的疗效。
研究参与者及时间:一项为期12周的随机临床试验,包括302例绝经后患有中度至重度症状的女性
研究什么(研究内容):主要结果为所报告的症状严重程度下降
如何研究(研究设计):这是一项随机临床试验(RCT)。随机临床试验可以对干预的真实效果做出最强有力的推论。 但是因为患者特征或其他变量可能与RCT研究中所用的不同,所以并非所有的RCT结果都可以在现实中被重复。
作者:Caroline M. Mitchell, M.D., 麻省总医院,波士顿,以及共同作者
研究结果:与安慰剂片剂加安慰剂凝胶相比,阴道雌二醇片剂加安慰剂凝胶以及阴道保湿剂加安慰剂片剂在改善症状严重程度或改善性功能方面并没有更好的效果。
研究局限:本研究结果的普遍性受到缺少多样性的研究人群的限制。
研究结论:我们需要更好地了解绝经后阴道症状的内在机制,以指导今后对治疗方案的改善。
欲了解更多详情并阅读完整的研究报告,请访问For The Media网站:https://media.jamanetwork.com/。
Treating Postmenopausal Vulvovaginal Symptoms in Women